Understanding Maternal Mortality Data and Terminology as an Advocacy Tool
By: Samantha Berg, MPH
Despite its wealth and high healthcare spending, the United States is deep in a maternal health crisis. As maternal health advocates, we understand the devastation of this crisis on families and communities and the urgent need for action. Yet we are often at the whim of decision-makers with limited funding and capacity, and competing priorities, when we advocate for policies and programs to address the problem. So, when we secure a meeting or even a minute of airtime with those key decision-makers, we need to make it count.
In advocacy, we know the effectiveness of pairing personal stories with data. Real-life stories pull at heartstrings and ground the issue in a relatable way, while data magnifies the issue and helps support our claims. And although we emphasize the importance of storytelling, we don’t always pay the same attention to choosing data that is both accurate and relevant. That’s why SMFM recently published “Assessing and using maternal mortality data,” which outlines the different types of data, their sources, and considerations and best practices for their use.
Appreciating Differences in Mortality Terminology and Definitions
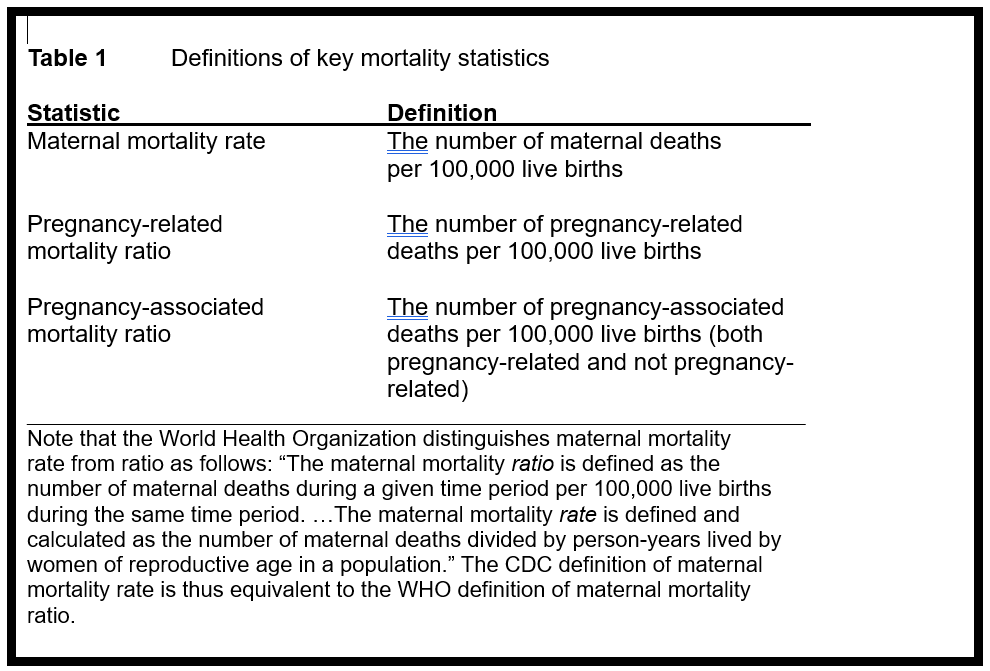
Although the term “maternal mortality” is often broadly used, there are actually three terms: maternal mortality, pregnancy-associated mortality, and pregnancy-related mortality. Each term has its own specific definition and data sources with accompanying benefits and drawbacks. Notably, these terms cannot be used interchangeably and should never be compared.
A maternal death is the death of a person while pregnant or within 42 days of the end of a pregnancy, regardless of the duration and site* of the pregnancy, and from any cause related to or aggravated by the pregnancy or its management. Maternal deaths do not include those from accidental or incidental causes, such as motor vehicle accidents or drug overdose. In the US, the best source for maternal death data is the National Vital Statistics System, or NVSS.
Maternal death data is useful in advocacy because it allows us to compare maternal health in the US to other countries. Without maternal death data, we wouldn’t know that the US ranks behind other high-income countries in maternal mortality rates, including Canada, the United Kingdom, and Japan.
|
While maternal death data is incredibly useful for cross-country comparisons, it does not provide a full understanding of the maternal health crisis. For a more complete picture, we must look at pregnancy-associated and pregnancy-related death data. A pregnancy-associated death is the death of a person during pregnancy or within one year postpartum, regardless of cause. This means pregnancy-associated mortality data includes deaths that are completely unrelated to pregnancy, like motor vehicle accidents, as well as deaths directly related to pregnancy. Pregnancy-associated deaths can be reviewed to determine their pregnancy-relatedness. |
 |
A pregnancy-associated death is the death of a person during pregnancy or within one year postpartum, regardless of cause. This means pregnancy-associated mortality data includes deaths that are completely unrelated to pregnancy, like motor vehicle accidents, as well as deaths directly related to pregnancy. Pregnancy-associated deaths can be reviewed to determine their pregnancy-relatedness.
A pregnancy-related death is a death during pregnancy or within one year postpartum from a pregnancy complication (eclampsia, for instance), chain of events initiated by pregnancy (such as postpartum depression), or the aggravation of an unrelated condition by the effects of pregnancy (such as lupus). This means that the deaths are causally related to pregnancy – so, unlike something like a motor vehicle accident, the person would not have died if they were not pregnant.
While pregnancy-associated mortality data is certainly useful in advocating for better policies and programs for pregnant people, it only establishes correlation, even when comparing instances of death to non-pregnant people. On the other hand, pregnancy-related mortality data has already established a causal relationship between the deaths and pregnancy and is thus a better tool for advocacy.
Pregnancy-Related Mortality Data Sources
In the US, there are two sources for pregnancy-related death data — the Pregnancy Mortality Surveillance System (PMSS) and maternal mortality review committees (MMRCs).
PMSS is a national surveillance system that tracks pregnancy-related deaths, collecting data from death certificates, medical records, and other sources to help identify trends, causes, and risk factors for pregnancy-related mortality.
With the use of pregnancy-related data from PMSS, advocates can highlight national-level information, including leading causes of death and major disparities by race-ethnicity. PMSS also helps us illustrate how the maternal health crisis is not improving. According to PMSS, there were 665 pregnancy-related deaths in 2024. The last time the number of pregnancy-related deaths fell below 600, it was in 2002. Below 500, it was 1998.
Although PMSS is the best source for painting a national picture of pregnancy-related mortality, MMRCs are best used to understand the crisis on a state or local level. As state or local multidisciplinary bodies, MMRCs look beyond medical records, reviewing social service records and sometimes conducting informant interviews with close contacts of those who have died. MMRCs also determine the preventability of deaths and develop recommendations to reduce future ones.
MMRCs can contribute their data to the Maternal Mortality Review Information App (MMRIA), a centralized data system overseen by the Centers for Disease Control and Prevention (CDC). Even though most states contribute data to MMRIA, CDC analyses of that data are not considered national, and thus should be used with careful consideration. However, this does not mean that they can’t be used in national conversations. In fact, MMRIA data can be used to help fill gaps left by PMSS. For example, PMSS lacks sufficient information to determine pregnancy-relatedness of injury deaths and does not include mental health as a leading cause of death. Advocates who want to bring attention to mental health and injury-related deaths can use MMRIA data, so long as we clarify that the data is only near-national.
Why Understanding the Different Types of Data Matters
Considering recent distrust of research, medical expertise, and data in general, it’s easy to feel frustrated and disheartened and think, “Why does this matter?” If folks aren’t listening, why put in the effort?
This distrust means that now, more than ever, we need to make sure our terminology and data are accurate and relevant to strengthen our credibility. Credibility helps us shore up our arguments and prevent misunderstanding in the conversation.
Additionally, a better understanding and utilization of the different types of data will help us develop appropriate interventions to address our maternal health crisis. Whether these interventions are programmatic or policy, understanding the data will help us ensure our resources and expertise are being properly allocated.
A comprehensive understanding of the different types of data and how they can be used will ultimately lead to more effective advocacy and solutions. Knowing where data comes from, why it’s important, and how it can be used will increase our confidence and make us more effective communicators and advocates for maternal health.
# # #
*The location where the fertilized egg has implanted (i.e., normal uterine implantation or ectopic).
Samantha Berg, MPH, is Senior Manager of Advocacy at SMFM.